Methods
Research Instrument, Sampling, and Data Collection
Data were collected using a self-administered survey from customers of relaxation bars in Lagos, Nigeria. Relaxation bars are leisure and recreational places that form a significant part of the growing Nigerian hospitality industry (Ogunmokun et al., 2020a). They are mostly outdoor relaxation centers with great natural and built environments, where drinks and light food are sold. They typically operate at night, and occasionally local African music bands perform live quietly. After obtaining the consent of the relaxation centers’ management, customers were intercepted as they leave the relaxation spot and were invited to participate in the survey. The data collection commenced in the last quarter of 2020; 3 weeks following the third phase of easing lockdown regulations (Ibrahim et al., 2020). Respondents were asked to reflect on their time at the relaxation bar, and honestly answer the questions in the questionnaire. They were assured anonymity and told that there were no wrong or right answers. A total of 213 customers voluntarily agreed to participate in the survey. See Table 1 for details of the samples’ demographic characteristics. All items were measured on a 5-point Likert scale; with 1 being Strongly disagree, and 5 being Strongly agree. The five sub-dimensions of therapeutic servicescape, with a total of 18 items were adapted from Rosenbaum et al. (2020). COVID stress was measured with 6 items adapted from Taylor et al. (2020), and revisit intention was measured with a 7-item scale adapted from Meng and Choi (2018).
Table 1: Sample Demographics 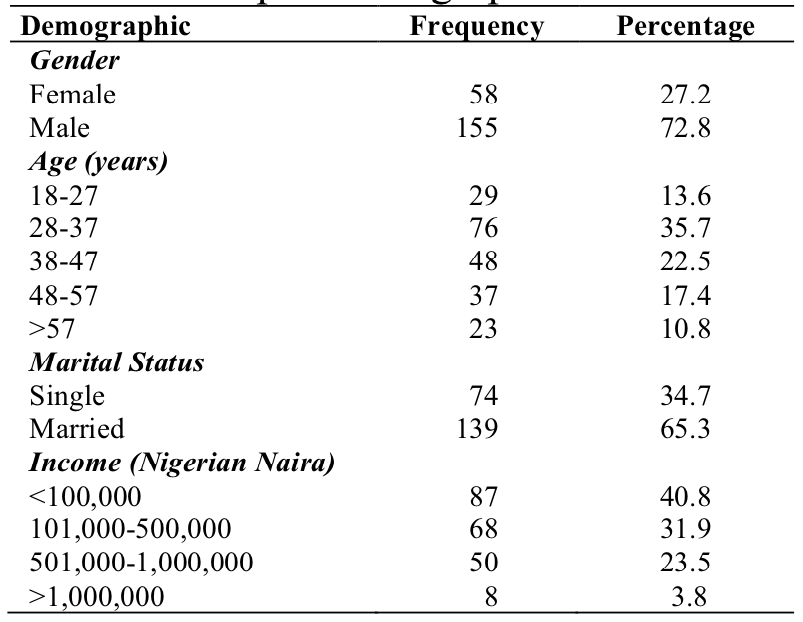
Data Analysis
Common Method Variance
There is a potential risk of common method bias as the data were collected from a single source. For this reason, some preventative measures were taken. First, in the questionnaire design, Viswanathan and Kayande’s (2012) recommendation on item sequencing across and within constructs was adopted, to prevent responds bias arising from respondents’ guessing the potential relationship between the study’s constructs. Second, we avoided ambiguous terminologies in the wording of the items, to enhance respondents’ understanding of the questions and be able to answer honestly. Finally, during the data collection, respondents were voluntarily recruited; they were guaranteed anonymity and assured that the data will be used strictly for statistical purposes. Posthoc, Harman single test factor was conducted, and it revealed that no single item had more than 50% of the total variance extracted (Podsakoff et al., 2003). Thus, common method bias does not seem to be an issue with the study’s data.
First-Order Measurement Model Assessment
For the sake of parsimony and on theoretical grounds, therapeutic servicescape is treated as a reflective second-order construct; with relational resources, fascination, being-away, cohesion, and scope as its sub-dimensions. Following the examples of Ogunmokun et al. (2021a), and Ogunmokun and Timur (2021), the Confirmatory Factor Analysis (CFA) of all first-order construct was conducted. CFA results revealed accepted fit indices for all first-order constructs (relational resources, fascination, being-away, cohesion, scope, COVID stress and revisit intention) - χ2 = 672.760, df = 328, Δdf = 2.051, CFI = .957, IFI = .957, SRMR = .060, RMSEA = .069. The CFA results also revealed accepted fit indices for second-order therapeutic servicescapes measured as a latent construct with five dimensions χ2 = 269.008, df = 129, Δdf = 2.085, CFI = .974, TLI = .969, SRMR = .045, RMSEA = .072. However, a CFA of one-factor model (with all items loading on one variable) revealed much poorer fit to data- χ2 = 3429.644, df = 349, Δdf = 9.827, CFI = .593, IFI = .595, SRMR = .158, RMSEA = .204. The convergent and discriminate validities of the first-order model were also tested, and they demonstrated satisfactory validities (see Table 2).
Table 2: First-Order Correlation and Validities 
Study’s Measurement Model
The CFA of the study’s constructs (COVID stress, revisit intention, and second-order therapeutic servicescape) revealed accepted fit indices- χ2 = 711.510, df = 341, Δdf = 2.087, CFI = .951, IFI = .951, SRMR = .065, RMSEA = .072. The constructs likewise demonstrated convergent validity as all factor loadings were significant and above .5 (Anderson & Gerbing, 1988), and values of the reliability test had Cronbach alpha > .70, confirming high reliability (see Table 3). Values of average variance extracted (AVE) were above .50, likewise, the values of the composite reliability are more than the values of the AVE, which confirms the convergent validity of the study’s model (Hair et al., 2010). Also, the values of MSV were less than the values of their respective AVE, further confirming the constructs’ discriminant validity (Hair et al., 2010) (see Table 4). To ensure the absence of multicollinearity, VIF values were checked, and they have values ranging from 1.40 to 1.56, which were below the acceptable threshold of 10.
Table 3: Factor Loadings, Means, and Distribution 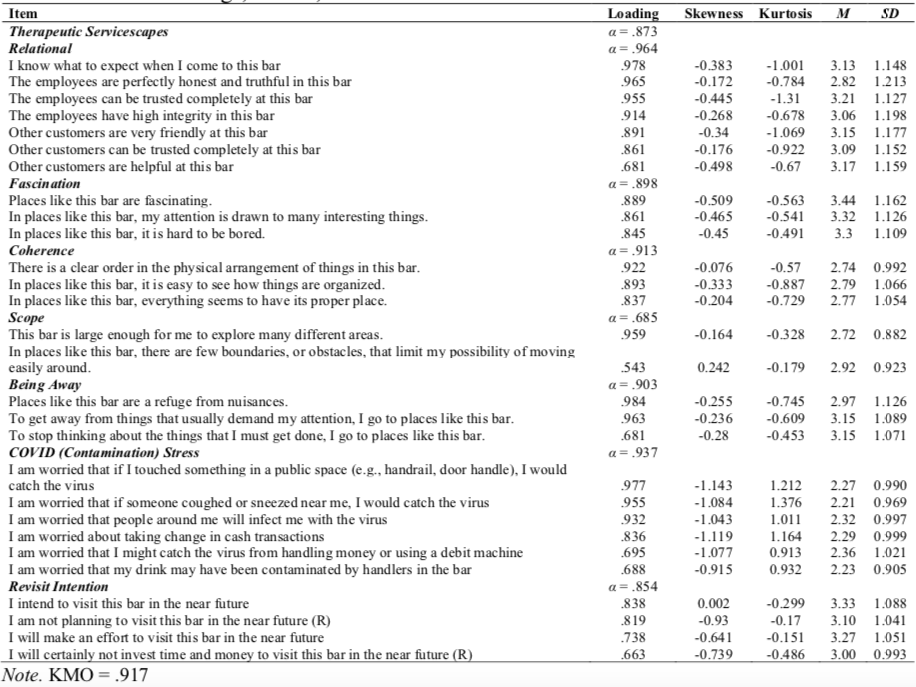
Table 4: Correlation and Validities 
Structural Model Assessment
The hypotheses positing the indirect and direct relationships of the study were estimated via the structural equation modeling technique (SEM) using a bootstrapping approach. This is most appropriate as there have been criticisms of the stepwise approach of testing mediation effects (Preacher & Hayes, 2004), as it does not directly assess indirect effects. Consequently, the study employs an SEM bootstrapping approach to test mediation because it estimates indirect effects, accommodates for assumptions of normality, provides the overall model fit, and assesses indirect and direct effects in a causal model.
Specifically, the study’s hypotheses were tested using SPSS AMOS24 with 10,000 bootstrapping at 95% confidence. Hypothesis 1 tested the relationship between therapeutic servicescape and COVID stress and found that there is a significant negative association (β = -.508; 95% CI [-.377, -.062]). Thus hypothesis 1 is supported. Hypothesis 2 tested the relationship between therapeutic servicescape and customers’ revisit intention and found that there is a significant association between them (β= .194; 95% CI [.039, .363]). Thus, hypothesis 2 is supported.
Mediation Analysis
Finally, hypothesis 3 tested the mediating role of COVID stressin the indirect relationship between therapeutic servicescape and customers’ revisit intention. The indirect effect from the bootstrap analysis was found to be positive and significant (ab = .204), with a 95% confidence interval not including zero (.110 to .317). Since the direct effect (c) hypothesized in hypothesis 2 is positive (.194) and significant (p = .0037), the study’s hypothesized mediation is complementary (Zhao et al., 2010). Thus, hypothesis 3 is supported.
Table 5: Summary of Hypotheses  ***
***